







Hemorrhoids
 Hemorrhoids, also spelled haemorrhoids, are vascular structures in the anal canal. In their normal state, they are cushions that help with stool control. They become a disease when swollen or inflamed; the unqualified term "hemorrhoid" is often used to mean the disease. The signs and symptoms of hemorrhoids depend on the type present. Internal hemorrhoids usually present with painless, bright red rectal bleeding when defecating. External hemorrhoids often result in pain and swelling in the area of the anus. If bleeding occurs it is usually darker. Symptoms frequently get better after a few days. A skin tag may remain after the healing of an external hemorrhoid.
Hemorrhoids, also spelled haemorrhoids, are vascular structures in the anal canal. In their normal state, they are cushions that help with stool control. They become a disease when swollen or inflamed; the unqualified term "hemorrhoid" is often used to mean the disease. The signs and symptoms of hemorrhoids depend on the type present. Internal hemorrhoids usually present with painless, bright red rectal bleeding when defecating. External hemorrhoids often result in pain and swelling in the area of the anus. If bleeding occurs it is usually darker. Symptoms frequently get better after a few days. A skin tag may remain after the healing of an external hemorrhoid.
While the exact cause of hemorrhoids remains unknown, a number of factors which increase pressure in the abdomen are believed to be involved. This may include constipation, diarrhea, and sitting on the toilet for a long time. Hemorrhoids are also more common during pregnancy. Diagnosis is made by looking at the area. Many people incorrectly refer to any symptom occurring around the anal area as "hemorrhoids" and serious causes of the symptoms should be ruled out. Colonoscopy or sigmoidoscopy is reasonable to confirm the diagnosis and rule out more serious causes.
Often, no specific treatment is needed. Initial measures consists of increasing fiber intake, drinking fluids to maintain hydration, NSAIDs to help with pain, and rest. Medicated creams applied to the area are poorly supported by evidence. A number of minor procedures may be performed if symptoms are severe or do not improve with conservative management. Surgery is reserved for those who fail to improve following these measures.
Half to two thirds of people have problems with hemorrhoids at some point in their lives. Males and females are affected about equally commonly. Hemorrhoids affect people most often between 45 and 65 years of age. It is more common among the wealthy. Outcomes are usually good. The first known mention of the disease is from a 1700 BC Egyptian papyrus.
Signs and symptoms
In about 40% of people with pathological hemorrhoids there are no significant symptoms. Internal and external hemorrhoids may present differently; however, many people may have a combination of the two. Bleeding enough to cause anemia is rare, and life-threatening bleeding is even more uncommon. Many people feel embarrassed when facing the problem and often seek medical care only when the case is advanced.
External
If not thrombosed, external hemorrhoids may cause few problems. However, when thrombosed, hemorrhoids may be very painful. Nevertheless, this pain typically resolves in two to three days. The swelling may, however, take a few weeks to disappear. A skin tag may remain after healing. If hemorrhoids are large and cause issues with hygiene, they may produce irritation of the surrounding skin, and thus itchiness around the anus.
Internal
 Internal hemorrhoids usually present with painless, bright red rectal bleeding during or following a bowel movement. The blood typically covers the stool (a condition known as hematochezia), is on the toilet paper, or drips into the toilet bowl. The stool itself is usually normally coloured. Other symptoms may include mucous discharge, a perianal mass if they prolapse through the anus, itchiness, and fecal incontinence. Internal hemorrhoids are usually only painful if they become thrombosed or necrotic.
Internal hemorrhoids usually present with painless, bright red rectal bleeding during or following a bowel movement. The blood typically covers the stool (a condition known as hematochezia), is on the toilet paper, or drips into the toilet bowl. The stool itself is usually normally coloured. Other symptoms may include mucous discharge, a perianal mass if they prolapse through the anus, itchiness, and fecal incontinence. Internal hemorrhoids are usually only painful if they become thrombosed or necrotic.
Causes
The exact cause of symptomatic hemorrhoids is unknown. A number of factors are believed to play a role, including irregular bowel habits (constipation or diarrhea), lack of exercise, nutritional factors (low-fiber diets), increased intra-abdominal pressure (prolonged straining, ascites, an intra-abdominal mass, or pregnancy), genetics, an absence of valves within the hemorrhoidal veins, and aging. Other factors believed to increase risk include obesity, prolonged sitting, a chronic cough, and pelvic floor dysfunction. Evidence for these associations, however, is poor.
During pregnancy, pressure from the fetus on the abdomen and hormonal changes cause the hemorrhoidal vessels to enlarge. The birth of the baby also leads to increased intra-abdominal pressures. Pregnant women rarely need surgical treatment, as symptoms usually resolve after delivery.
Pathophysiology
Hemorrhoid cushions are a part of normal human anatomy and become a pathological disease only when they experience abnormal changes. There are three main cushions present in the normal anal canal. These are located classically at left lateral, right anterior, and right posterior positions. They are composed of neither arteries nor veins, but blood vessels called sinusoids, connective tissue, and smooth muscle. Sinusoids do not have muscle tissue in their walls, as veins do. This set of blood vessels is known as the hemorrhoidal plexus.
Hemorrhoid cushions are important for continence. They contribute to 15–20% of anal closure pressure at rest and protect the internal and external anal sphincter muscles during the passage of stool. When a person bears down, the intra-abdominal pressure grows, and hemorrhoid cushions increase in size, helping maintain anal closure. Hemorrhoid symptoms are believed to result when these vascular structures slide downwards or when venous pressure is excessively increased. Increased internal and external anal sphincter pressure may also be involved in hemorrhoid symptoms. Two types of hemorrhoids occur: internals from the superior hemorrhoidal plexus and externals from the inferior hemorrhoidal plexus. The dentate line divides the two regions.
Diagnosis
Hemorrhoids are typically diagnosed by physical examination. A visual examination of the anus and surrounding area may diagnose external or prolapsed hemorrhoids. A rectal exam may be performed to detect possible rectal tumors, polyps, an enlarged prostate, or abscesses. This examination may not be possible without appropriate sedation because of pain, although most internal hemorrhoids are not associated with pain. Visual confirmation of internal hemorrhoids may require anoscopy, insertion of a hollow tube device with a light attached at one end. The two types of hemorrhoids are external and internal. These are differentiated by their position with respect to the dentate line. Some persons may concurrently have symptomatic versions of both. If pain is present, the condition is more likely to be an anal fissure or an external hemorrhoid rather than an internal hemorrhoid.
Internal
 Internal hemorrhoids originate above the dentate line. They are covered by columnar epithelium, which lacks pain receptors. They were classified in 1985 into four grades based on the degree of prolapse:
Internal hemorrhoids originate above the dentate line. They are covered by columnar epithelium, which lacks pain receptors. They were classified in 1985 into four grades based on the degree of prolapse:
- Grade I: No prolapse, just prominent blood vessels
- Grade II: Prolapse upon bearing down, but spontaneous reduction
- Grade III: Prolapse upon bearing down requiring manual reduction
- Grade IV: Prolapse with inability to be manually reduced.
External
External hemorrhoids occur below the dentate or pectinate line. They are covered proximally by anoderm and distally by skin, both of which are sensitive to pain and temperature.
Differential
Many anorectal problems, including fissures, fistulae, abscesses, colorectal cancer, rectal varices, and itching have similar symptoms and may be incorrectly referred to as hemorrhoids. Rectal bleeding may also occur owing to colorectal cancer, colitis including inflammatory bowel disease, diverticular disease, and angiodysplasia. If anemia is present, other potential causes should be considered. Other conditions that produce an anal mass include skin tags, anal warts, rectal prolapse, polyps, and enlarged anal papillae. Anorectal varices due to increased portal hypertension (blood pressure in the portal venous system) may present similar to hemorrhoids but are a different condition. Portal hypertension does not increase the risk of hemorrhoids.
Prevention
A number of preventative measures are recommended, including avoiding straining while attempting to defecate, avoiding constipation and diarrhea either by eating a high-fiber diet and drinking plenty of fluid or by taking fiber supplements, and getting sufficient exercise. Spending less time attempting to defecate, avoiding reading while on the toilet, and losing weight for overweight persons and avoiding heavy lifting are also recommended.
Management
Conservative
Conservative treatment typically consists of foods rich in dietary fiber, intake of oral fluids to maintain hydration, nonsteroidal anti-inflammatory drugs, sitz baths, and rest. Increased fiber intake has been shown to improve outcomes and may be achieved by dietary alterations or the consumption of fiber supplements. Evidence for benefits from sitz baths during any point in treatment, however, is lacking. If they are used, they should be limited to 15 minutes at a time.
While many topical agents and suppositories are available for the treatment of hemorrhoids, little evidence supports their use. Steroid-containing agents should not be used for more than 14 days, as they may cause thinning of the skin. Most agents include a combination of active ingredients. These may include a barrier cream such as petroleum jelly or zinc oxide, an analgesic agent such as lidocaine, and a vasoconstrictor such as epinephrine. Some contain Balsam of Peru to which certain people may be allergic.
Flavonoids are of questionable benefit, with potential side effects. Symptoms usually resolve following pregnancy; thus active treatment is often delayed until after delivery.
Procedures
A number of office-based procedures may be performed. While generally safe, rare serious side effects such as perianal sepsis may occur.
- Rubber band ligation is typically recommended as the first-line treatment in those with grade 1 to 3 disease. It is a procedure in which elastic bands are applied onto an internal hemorrhoid at least 1 cm above the dentate line to cut off its blood supply. Within 5–7 days, the withered hemorrhoid falls off. If the band is placed too close to the dentate line, intense pain results immediately afterwards. Cure rate has been found to be about 87%with a complication rate of up to 3%.
- Sclerotherapy involves the injection of a sclerosing agent, such as phenol, into the hemorrhoid. This causes the vein walls to collapse and the hemorrhoids to shrivel up. The success rate four years after treatment is about 70%.
- A number of cauterization methods have been shown to be effective for hemorrhoids, but are usually only used when other methods fail. This procedure can be done using electrocautery, infrared radiation, laser surgery, or cryosurgery. Infrared cauterization may be an option for grade 1 or 2 disease. In those with grade 3 or 4 disease, reoccurrence rates are high.
Surgery
A number of surgical techniques may be used if conservative management and simple procedures fail. All surgical treatments are associated with some degree of complications including bleeding, infection, anal strictures and urinary retention, due to the close proximity of the rectum to the nerves that supply the bladder. Also, a small risk of fecal incontinence occurs, particularly of liquid, with rates reported between 0% and 28%.Mucosal ectropion is another condition which may occur after hemorrhoidectomy (often together with anal stenosis). This is where the anal mucosa becomes everted from the anus, similar to a very mild form of rectal prolapse.
- Excisional hemorrhoidectomy is a surgical excision of the hemorrhoid used primarily only in severe cases. It is associated with significant postoperative pain and usually requires 2–4 weeks for recovery. However, the long-term benefit is greater in those with grade 3 hemorrhoids as compared to rubber band ligation. It is the recommended treatment in those with a thrombosed external hemorrhoid if carried out within 24–72 hours. Glyceryl trinitrate ointment after the procedure helps both with pain and healing.
- Doppler-guided, transanal hemorrhoidal dearterialization is a minimally invasive treatment using an ultrasound doppler to accurately locate the arterial blood inflow. These arteries are then "tied off" and the prolapsed tissue is sutured back to its normal position. It has a slightly higher recurrence rate, but fewer complications compared to a hemorrhoidectomy.
- Stapled hemorrhoidectomy, also known as stapled hemorrhoidopexy, involves the removal of much of the abnormally enlarged hemorrhoidal tissue, followed by a repositioning of the remaining hemorrhoidal tissue back to its normal anatomical position. It is generally less painful and is associated with faster healing compared to complete removal of hemorrhoids. However, the chance of symptomatic hemorrhoids returning is greater than for conventional hemorroidectomy, so it is typically only recommended for grade 2 or 3 disease
Anal fistula
Anal fistula (plural fistulae), or fistula-in-ano, is a chronic abnormal communication between the epithelialised surface of the anal canal and (usually) the perianal skin. An anal fistula can be described as a narrow tunnel with its internal opening in the anal canal and its external opening in the skin near the anus. Anal fistulae commonly occur in people with a history of anal abscesses. They can form when anal abscesses do not heal properly.
Anal fistulae originate from the anal glands, which are located between the internal and external anal sphincter and drain into the anal canal. If the outlet of these glands becomes blocked, an abscess can form which can eventually extend to the skin surface. The tract formed by this process is a fistula.
Abscesses can recur if the fistula seals over, allowing the accumulation of pus. It can then extends to the surface again - repeating the process.
Anal fistulae per se do not generally harm, but can be very painful, and can be irritating because of the drainage of pus (it is also possible for formed stools to be passed through the fistula). Additionally, recurrent abscesses may lead to significant short term morbidity from pain and, importantly, create a starting point for systemic infection.
Treatment, in the form of surgery, is considered essential to allow drainage and prevent infection. Repair of the fistula itself is considered an elective procedure which many patients opt for due to the discomfort and inconvenience associated with an actively draining fistula.
Types
Depending on their relationship with the internal and external sphincter muscles, fistulae are classified into five types:

- Extrasphincteric fistulae begin at the rectum or sigmoid colon and proceed downward, through the levator ani muscle and open into the skin surrounding the anus. Note that this type does not arise from the dentate line (where the anal glands are located). Causes of this type could be from a rectal, pelvic or supralevator origin, usually secondary to Crohn's disease or an inflammatory process such as appendiceal or diverticular abscesses.
- Suprasphincteric fistulae begin between the internal and external sphincter muscles, extend above and cross the puborectalis muscle, proceed downward between the puborectalis and levator ani muscles, and open an inch or more away from the anus.
- Transphincteric fistulae begin between the internal and external sphincter muscles or behind the anus, cross the external sphincter muscle and open an inch or more away from the anus. These may take a 'U' shape and form multiple external openings. This is sometimes termed a 'horseshoe fistula.'
- Intersphincteric fistulae begin between the internal and external sphincter muscles, pass through the internal sphincter muscle, and open very close to the anus.
- Submucosal fistulae pass superficially beneath the submucosa and do not cross either sphincter muscle.
Signs and symptoms
Anal fistulae can present with the following symptoms:
- skin maceration
- pus, serous fluid and/or (rarely) feces discharge — can be bloody or purulent
- pruitus ani — itching
- depending on presence and severity of infection:
- pain
- swelling
- tenderness
- fever
Diagnosis
Diagnosis is by examination, either in an outpatient setting or under anaesthesia (referred to as EUA — Examination Under Anaesthesia). The fistula may be explored by using a fistula probe (a narrow instrument). In this way, it may be possible to find both openings. The examination can be an anoscopy. Diagnosis may be aided by performing a fistulogram, proctoscopy and/or sigmoidoscopy.
Possible findings:
- The opening of the fistula onto the skin may be observed
- The area may be painful on examination
- There may be redness
- An area of induration may be felt — thickening due to chronic infection
- A discharge may be seen
Differential diagnosis
Other conditions in which infected perianal "holes" or openings may appear include Pilonidal cysts/sinuses.
Treatment
There are several stages to treating an anal fistula:
Definitive treatment of a fistula aims to stop it recurring. Treatment depends on where the fistula lies, and which parts of the internal and external anal sphincters it crosses.
There are several options:
- Doing nothing
- Lay-open of fistula-in-ano
- Cutting seton
- Colostomy
- Fibrin glue injection
- FISTULOTOMY
- Fistula plug
- Endorectal advancement flap
- Fistula clip closure (OTSC Proctology)
- PERFACT Procedure
- LIFT Technique
- Seton stich
Anal fissure
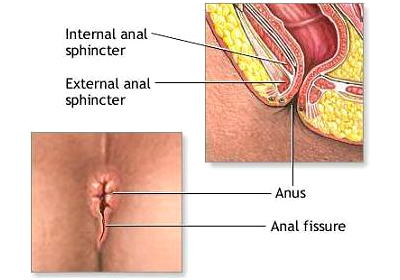 An anal fissure or rectal fissure is a break or tear in the skin of the anal canal. Anal fissures may be noticed by bright red anal bleeding on toilet paper,
An anal fissure or rectal fissure is a break or tear in the skin of the anal canal. Anal fissures may be noticed by bright red anal bleeding on toilet paper,
sometimes in the toilet. If acute they may cause pain after defecation,but with chronic fissures pain intensity is often less. Anal fissures usually extend from the anal opening and are usually located posteriorly in the midline, probably because of the relatively unsupported nature and poor perfusion of the anal wall in that location. Fissure depth may be superficial or sometimes down to the underlying sphincter muscle.
Causes
Most anal fissures are caused by stretching of the anal mucosa beyond its capability.
Superficial or shallow anal fissures look much like a paper cut, and may be hard to detect upon visual inspection, they will generally self-heal within a couple of weeks. However, some anal fissures become chronic and deep and will not heal. The most common cause of non-healing is spasming of the internal anal sphincter muscle which results in impaired blood supply to the anal mucosa. The result is a non-healing ulcer, which may become infected by fecal bacteria. In adults, fissures may be caused by constipation, the passing of large, hard stools, or by prolonged diarrhea. In older adults, anal fissures may be caused by decreased blood flow to the area. When fissures are found laterally, tuberculosis, occult abscesses, leukemic infiltrates, carcinoma, acquired immunodeficiency syndrome (AIDS) or inflammatory bowel disease should be considered as causes. Some sexually transmitted infections can promote the breakdown of tissue resulting in a fissure. Examples of sexually transmitted infections that may affect the anorectal area are syphilis, herpes, chlamydia and human papilloma virus.
Other common causes of anal fissures include:
- childbirth trauma in women
- Sexual Activities
- Crohn's disease
- ulcerative colitis
- poor toileting in young children.
Prevention
For adults, the following may help prevent anal fissures:
- Avoiding straining when defecating. This includes treating and preventing constipation by eating food rich in dietary fiber, drinking enough water, occasional use of a stool softener, and avoiding constipating agents. Similarly, prompt treatment of diarrhea may reduce anal strain.
- Careful anal hygiene after defecation, including using soft toilet paper and/or cleaning with water, plus the use of sanitary wipes.
- In cases of pre-existing or suspected fissure, use of a lubricating ointment (It is important to note that hemorrhoid ointment is contraindicated because it constricts small blood vessels, thus causes a decrease in blood flow, which prevents healing.)
In infants, frequent diaper change can prevent anal fissure. As constipation can be a cause, making sure the infant is drinking enough fluids (i.e. breastmilk, proper ratios when mixing formulas). In infants, once an anal fissure has occurred, addressing underlying causes is usually enough to ensure healing occurs.
Treatment
Non-surgical treatments are recommended initially for acute and chronic anal fissures. These include topical nitroglycerin or calcium channel blockers (e.g. diltiazem), or injection of botulinum toxin into the anal sphincter.
Other measures include warm sitz baths, topical anesthetics, high-fiber diet and stool softeners.
Medication
Local application of medication to relax the sphincter muscle, thus allowing the healing to proceed, was first proposed in 1994 with nitroglycerine ointment, and then calcium channel blockers in 1999 with nifedipine ointment, and the following year with topical diltiazem. Branded preparations are now available of topical nitroglycerine ointment (Rectogesic (Rectiv) as 0.2% in Australia and 0.4% in UK and US), topical nifedipine 0.3% with lidocaine 1.5% ointment (Antrolin in Italy since April 2004) and diltiazem 2% (Anoheal in UK, although still in Phase III development). A common side effect drawback of nitroglycerine ointment is headache, caused by systemic absorption of the drug, which limits patient acceptability.
A combined surgical and pharmacological treatment, administered by colorectal surgeons, is direct injection of botulinum toxin (Botox) into the anal sphincter to relax it. This treatment was first investigated in 1993. However, in many cases involving Botox injections the patients eventually had to choose another cure as the injections proved less and less potent, spending thousands of dollars in the meantime for a partial cure. Lateral sphincterotomy is the Gold Standard for curing this affliction. Combination of medical therapies may offer up to 98% cure rates.
Surgery
Surgical procedures are generally reserved for people with anal fissure who have tried medical therapy for at least one to three months and have not healed. It is not the first option in treatment.
The main concern with surgery is the development of anal incontinence. Anal incontinence can include inability to control gas, mild fecal soiling, or loss of solid stool. Some degree of incontinence can occur in up to 45 percent of patients in the immediate surgical recovery period. However, incontinence is rarely permanent and is usually mild. The risk should be discussed with one's surgeon.
Surgical treatment, under general anaesthesia, was either anal stretch (Lord's operation) or lateral sphincterotomy where the internal anal sphincter muscle is incised. Both operations aim to decrease sphincter spasming and thereby restore normal blood supply to the anal mucosa. Surgical operations involve a general anaesthetic and can be painful postoperatively. Anal stretch is also associated with anal incontinence in a small proportion of cases and thus sphincterotomy is the operation of choice.
Lateral internal sphincterotomy
Lateral internal sphincterotomy (LIS) is the surgical procedure of choice for anal fissures due to its simplicity and its high success rate (~95%). In this procedure the internal anal sphincter is partially divided in order to reduce spasming and thus improve the blood supply to the perianal area. This improvement in the blood supply helps to heal the fissure, and the weakening of the sphincter is also believed to reduce the potential for recurrence. The procedure is generally performed as a day surgery after the patient is given general anesthesia. The pain from the sphincterotomy is usually mild and is often less than the pain of the fissure itself. Patients often return to normal activity within one week.
LIS does, however, have a number of potential side effects including problems with incision site healing and incontinence to flatus and faeces (some surveys of surgical results suggest incontinence rates of up to 36%).
Though lateral internal sphincterotomy (LIS) is considered safe on short-term basis, there are concerns about its long-term safety. Pankaj Garg et al. published a systematic review and meta-analysis in which they analyzed the long-term continence disturbance two years after the LIS procedure. They found the incidence of long-term continence disturbance to be 14%, so caution and careful patient selection are needed before undergoing LIS.
Anal dilation
Anal dilation, or stretching of the anal canal (Lord's operation), has fallen out of favour in recent years, primarily due to the unacceptably high incidence of fecal incontinence. In addition, anal stretching can increase the rate of flatus incontinence.
In the early 1990s, however, a repeatable method of anal dilation proved to be very effective and showed a very low incidence of side effects. Since then, at least one other controlled, randomized study has shown there to be little difference in healing rates and complications between controlled anal dilation and LIS, while another has again shown high success rates with anal dilation coupled with low incidence of side effects.